|
Ivano Franko Hospital Tour July 11 th 2006
Today I visited the Ivano-Franko City Hospital. Yesterday through 2 Ukrainian teachers, Oksana and Lesia I was introduced to the Vice Mayor of Ivano Frankysk whothen facilitated a meeting with the cityhospital administrator and he accepted some simple medical supplies given to me by Hope International. He gave me a contact number so that interested Canadian doctors and nurses could enquire about doing future visits. Also medical students could consider rotations here as well. My interpreter Lena and I visited the Pediatric, Obstetric and Polyclinic centres. Lena learned as much about Ukrainian health care as I did. Pediatric HospitalWe visited the various wards and laboratories. The x-ray equipment was old, but serviceable. It was a large room but all the window shutters, walls and doors were shielded with lead. Since Chernobyl Ukrainians are very aware of radiation effects. Lena told me that since Chernobyl, in her opinion, the rate of cancers had increased, even in areas such as Ivano-Franko, far removed from the actual Chernobyl site. She also said that malignancy remains one of the main causes of death among Ukrainians. Interestingly many studies deny this and claim Ukrainians are over sensitive about radiation illnesses but I find this hard to believe after touring the Chernobyl museum. The pediatric wards were under construction as we toured them.
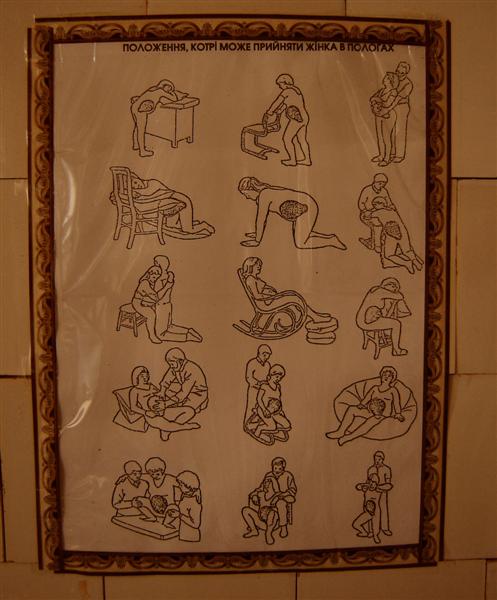
Maternity HospitalWe traveled to a new building and our physician guide explained that he would take us through just as a Ukrainian pregnant woman would move through the hospital so Lena and I gowned up and entered the maternity ward. According to my understanding there were about 1,200 births in the last six months with 3-4 fetal deaths. I had heard another statistic of 17 deaths per year though. The average term infant weight would range from 2.2 kg4kg. I am sure the Canadian birth weights are higher, with a greater incidence of gestational diabetes in our Canadian women. Our doctor explained that the greatest problems included anemia and poor lung development. We wore a white laboratory coat and white booties to cover our street shoes. As observers Lena and I would enter the wards in proper attire. We entered an obstetric elevator which had a small cot and a box with some medication in it. I have never seen anyone who had thought to put a bed inside an elevator but this struck me as a very good idea. There was just enough space for an attendant to attend a delivery at the foot of the bed. The doctor assured me though that the elevator had never become stuck and no deliveries had occurred inside. We next went to the general labour and delivery floor. A woman was in labour and was screaming. I believe this upset Lena but his would be no different from an obstetrical ward anywhere in the world. We toured some of the vacant birthing rooms. Interestingly, under Ukrainian law the laboring woman is allowed many choices (e.g. her choice of analgesia and position of birth). A poster showed fifteen possible positions for birthing.
Birthing positions This is something very new to me as when I did my obstetric rotation the senior obstetric professors admitted that they did not have much experience beyond the standard lithotomy position (this position is so named because the position of lying on the back with the legs apart is the same used by patients needing kidney stones removed, litho=stones).
picture of birthing room chair A midwife attends all deliveries but doctors are also available. I met one of the anesthesiologists in the hall and he told me that spinal analgesia with lidocaine and inhalational nitrous oxide are a popular choice of analgesia. Endotrachial intubation is required Fentanyl is used but Demerol and morphine were not used, nor was ketamine. Fentanyl is a much better drug for anesthesia than Demerol and it was interesting to see that even in a poor system they were using good choices. We passed the high-risk area and saw one woman being prepped for caesarian section. Because she had had two prior caesarian sections and was having another she needed special preparation so that the old scars did not break apart. We also visited the pre-labour floor where women with pathologies were admitted prior to birthing. The post-labour floor had less supplies for the new moms and babies. Husbands were allowed to visit these rooms but were not allowed to visit outside of certain hours. Husbands were also invited to attend low-risk deliveries but not risk ones, which is the same as I remember in Canada.
Exercise ball for pain relief In all of the rooms a pictogram was drawn with a baby bottle of milk with a line drawn through it, reinforcing the message that breast-feeding was strongly encouraged. After normal vaginal delivery the expected length of stay was three days and it was eight days for post-caesarian. We went to an educational room where a picture of the Virgin Mary breast-feeding baby Jesus reinforced the message of breast-feeding from the highest authority. Throughout the hospital positive images of the family, father, mother, and child were displayed. Breastfeeding was done openly although I believe, from one of my ethnographic nursing reference books, that this is not done publicly after discharge.
The hospital also had a room where daily education on breast-feeding was provided. Education was begun in the polyclinic (which we would later visit) and continued after the birth. The ten rules of breast-feeding hung prominently in that room mirroring the importance of the Ten Commandments. I didn't get a full translation, but they included allowing breast-feeding on demand for infants (replacing the previously recommended scheduled feedings) and not allowing non-breast milk substitutes such as milk or formula to replace breast milk. Both the educators and doctors had never heard of the La Leche league though. I further amused the doctor by telling him of how two babies had been switched at birth in Winnipeg and even breast-fed by the wrong mother. As I expected he was shocked and said that in his twenty years of practice he had never heard of such a thing. New mothers are also paired with an attendant, either a relative or nurse, (medical sister) who remains with them during their stay. Lastly we were introduced to a parallel wing of the hospital that separated to attend women with infection such as tuberculosis, HIV, and even chlamydia. We also visited the neonatal intensive care ward, which was empty, but the assistant director explained that it was still deficient in lacking one incubator. PolyclinicWe next visited the polyclinic or outpatient department. As usual Lena and I would meet with the administrator and then be given a tour by one of his assistants. Our guide was a pleasant nurse who cheerfully showed us the sections.
The laboratories were as I expected them to be-separate departments for urinalysis, cytology and chemistry. The x-ray department was equipped with tomography programming, which can give better information than plain x-rays. In Canada since we use Computer Tomography (CT scans) we seldom use tomograms. The problem with tomograms is to get a defined image you shoot x-rays from multiple angles of the body, but this means more radiation exposure. CT scans give much better images but are of course very expensive relative to tomograms. We visited the ophthalmologists who still used a working Soviet produced slit lamp and manual tonometers to measure glaucoma but I observed the Snell eye chart was of course in Ukrainian Cyrillic characters, not Russian. Most equipment throughout the polyclinic was no longer Russian except for the Slit lamp and x-ray machines. The dentist was very modern and took some time from his patient to greet me. He was the only office I saw that used a computer except for the epidemiological department. We met two gynecologists, who were both women, this being an exclusively female occupation. Interestingly as we entered the gynecology office an angry old woman who had been waiting followed us in, I suppose she thought that I was trying to cut in line. The examining chair allowed the woman to partially sit up with legs abducted. This is probably a much more comfortable position for women than an examining bed design. This is likely because the gynecologists themselves are women. We observed a physical rehabilitation center-most commonly used for post-heart attacks and severe respiratory illnesses. Patients are prescribed specific exercises under the supervision of an athletics instructor and physician. Another room was used for cardio stress testing. There were many physical therapists. They also showed me some of their rehabilitation equipment including therapeutic ultrasound and laser and magnet therapy. One room subdivided with curtains also had several massage therapists working. Adjacent to the women's clinic was the men's clinic. Our nurse guide commented that although he is very young he is very good. As in Canada everyone likes to tease young doctors. We visited a young woman, dressed in colorful yellow, who was instructing a young pregnant mother on breast-feeding. I am not sure if she was also a nurse but was dressed more casually to get a better rapport with the patients. She explained that she used art therapy in conjunction with her teachings. She had an aquarium filled with sand and toys. She also had several of the S or Swiss exercise balls in her office. These were also used during labour to relieve pain by having the laboring woman sit on these. AIDS clinicWe briefly visited the infectious disease clinic. Many of their patients are HIV or SNEAD, as everyone translates it into Ukrainian. Lena said there were mostly young teenagers who were ill. The hospital wards were very close together and there wasn't as much confidentiality as you would expect in a western hospital. If you were seen in an infectious disease line up I am sure people may think you had HIV. I didn't get the opportunity to ask about HIV detection, prevention, or treatment. HIV is very high in Ukraine and is over 10 times the incidence of the rest of Europe. I really appreciated this gracious tour of the City hospital Doctors and nurses wishing o do rotations may contact me for more information
Staff
of Ivano Frankysk accepting medical supplies from Hope International
|